
 +919325609388
+919325609388
Anterior vs Posterior Shoulder Dislocation: Quick Comparison
If you’ve ever had a shoulder “pop out,” you know how alarming it feels. But not all shoulder dislocations are the same. When comparing anterior vs posterior shoulder dislocation, the key difference lies in which direction the upper arm bone (humerus) moves out of the socket. In an anterior dislocation, the bone slips forward — and this accounts for nearly 95% of all shoulder dislocations. In a posterior dislocation, the bone shifts backward, which is far rarer but often more difficult to diagnose.
Understanding the difference matters — not just for doctors and physiotherapists, but for anyone who has experienced a shoulder injury and wants to know what’s really going on. At Healyos Physiotherapy, we see both types of dislocations at our Pune clinic and through our at-home physiotherapy services, and early, accurate identification is the first step toward effective recovery.
What Exactly Is a Shoulder Dislocation?
The shoulder is the most mobile joint in your body — and that mobility comes at a cost. The ball-shaped head of the humerus sits in a shallow cup called the glenoid cavity, held in place by muscles, tendons, and ligaments. When a force is strong enough to push that ball out of the cup, a dislocation occurs.
There are two main directions this can happen:
- Anterior (forward) — by far the most common
- Posterior (backward) — rare but frequently missed on initial assessment
There are also inferior dislocations (downward), but these are extremely uncommon and beyond the scope of this comparison.
Anterior Shoulder Dislocation: The Common One
How Does It Happen?
Anterior dislocations typically occur when the arm is in an abducted and externally rotated position — think of falling on an outstretched hand, a tackle in sports, or a direct blow to the back of the shoulder.
Who Gets It?
- Athletes in contact sports (rugby, football, wrestling)
- Young adults and active individuals
- People who’ve had a previous dislocation (recurrence is common)
What Does It Look Like?
When the humeral head slides forward, the shoulder takes on a distinctive “squared-off” appearance. The natural rounded shape of the shoulder disappears, and there may be a visible bulge at the front of the joint.
Classic signs of anterior dislocation:
- Arm held slightly away from the body in external rotation
- Flattening of the deltoid muscle (squared-off look)
- Severe pain and muscle spasm
- Restricted movement in almost all directions
- Numbness or tingling in the arm (if the axillary nerve is involved)
Posterior Shoulder Dislocation: The Missed One
How Does It Happen?
This is where things get interesting — and where misdiagnosis is most likely. Posterior shoulder dislocation typically results from:
- A seizure (the most common non-traumatic cause — violent muscle contractions force the head backward)
- Electric shock
- A direct force to the front of the shoulder
- A fall with the arm flexed and internally rotated
Why Is It So Often Missed?
Posterior dislocations are notoriously easy to overlook. On a standard AP (front-facing) X-ray, the joint can appear almost normal to an untrained eye. Studies suggest that up to 50–79% of posterior dislocations are initially missed, sometimes for weeks or months. This is one reason understanding anterior vs posterior shoulder dislocation on X-ray findings is so critical in clinical settings.
What Does It Look Like?
The shoulder may appear less dramatically deformed than with an anterior dislocation, which contributes to delayed diagnosis.
Classic signs of posterior dislocation:
- Arm held in internal rotation and adduction (pressed against the body)
- Loss of the normal contour of the shoulder (but subtler than anterior)
- Inability to externally rotate the arm — this is a hallmark sign
- Pain that worsens with any attempt at external rotation
- The shoulder may look “normal” from the front
Anterior and Posterior Shoulder Dislocation: Side-by-Side Comparison
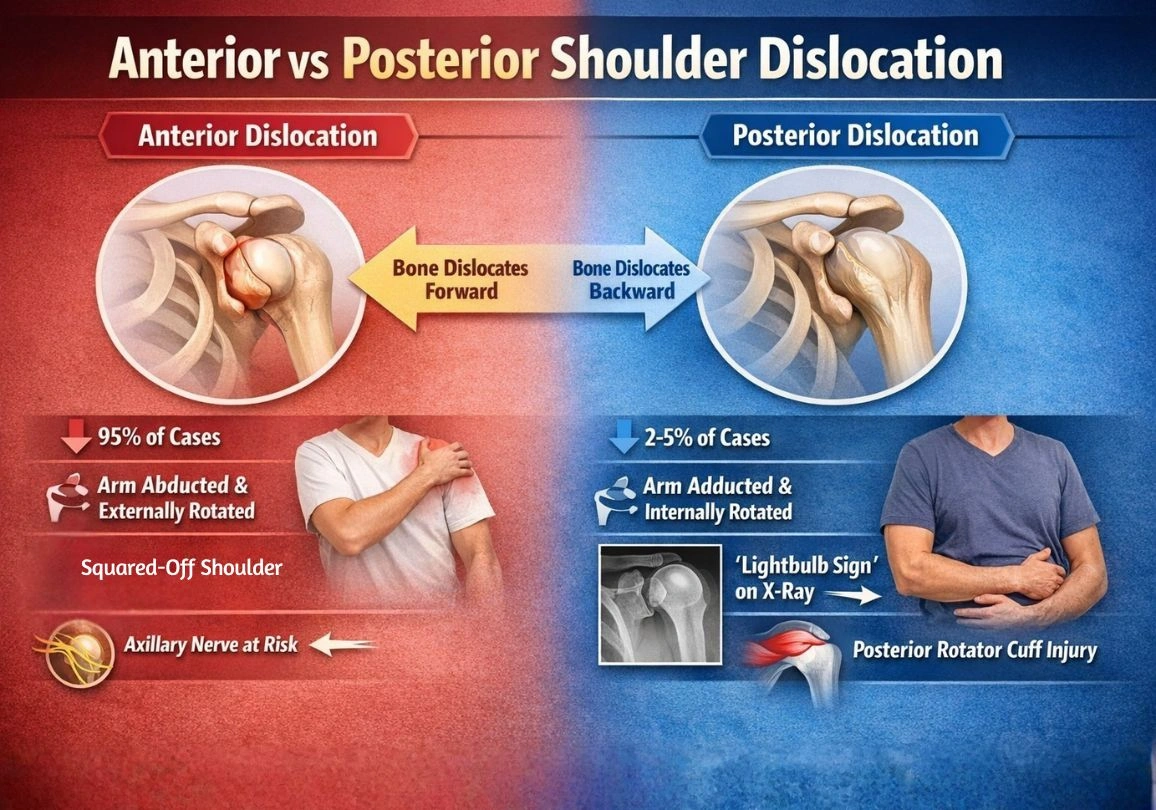
| Feature | Anterior Dislocation | Posterior Dislocation |
| Frequency | ~95% of cases | ~2–5% of cases |
| Mechanism | Abduction + external rotation | Seizure, electric shock, direct blow |
| Arm Position | Externally rotated, abducted | Internally rotated, adducted |
| Shoulder Appearance | Squared-off, prominent acromion | Subtle deformity, less obvious |
| Key Clinical Sign | Loss of rounded shoulder shape | Inability to externally rotate |
| Nerve at Risk | Axillary nerve | Posterior rotator cuff |
| Diagnosis Difficulty | Easier to identify | Frequently missed |
| Associated Injury | Bankart lesion, Hill-Sachs lesion | Reverse Hill-Sachs lesion |
Anterior vs Posterior Shoulder Dislocation on X-Ray
This is one of the most clinically important aspects of comparing these two conditions. Anterior vs posterior shoulder dislocation radiology findings can look very different — or surprisingly similar.
Anterior Dislocation on X-Ray
On a standard AP view, the diagnosis is usually straightforward:
- The humeral head is clearly visible below and medial to the glenoid
- There may be a Hill-Sachs lesion — a compression fracture on the back of the humeral head caused by it striking the rim of the glenoid
- A Bankart lesion (damage to the anterior glenoid labrum) may also be detected, though this often requires MRI
Posterior Dislocation on X-Ray
This is where anterior vs posterior shoulder dislocation on X-ray becomes a real diagnostic challenge:
- The humeral head may overlap with the glenoid on a standard AP view, appearing almost normal
- A key sign is the “lightbulb sign” — the internally rotated humerus looks rounded and symmetrical, like a lightbulb, rather than having its normal teardrop profile
- There may be a reverse Hill-Sachs lesion (also called a McLaughlin lesion) — a compression fracture on the front of the humeral head
- The “trough line” (a vertical dense line at the medial humeral head) is another tell-tale sign
A Y-view or axillary lateral X-ray is essential to confirm a posterior dislocation. This is why many guidelines now recommend obtaining two views at a minimum whenever a shoulder dislocation is suspected.
Clinical Pearl: If a patient presents with a shoulder injury after a seizure and cannot externally rotate their arm, a posterior dislocation should be suspected until proven otherwise — even if the AP X-ray looks normal.
Treatment: What Happens After Diagnosis?
Regardless of type, the first step is reduction — getting the humeral head back into the socket. This is done by a trained clinician, usually in an emergency setting, often with sedation or analgesia.
After Reduction: Where Physiotherapy Becomes Essential
Once the shoulder is back in place, the real work begins. A dislocation — whether anterior or posterior — leaves behind damaged soft tissue, weakened muscles, and a joint that’s now at higher risk of dislocating again.
At Healyos Physiotherapy, our post-dislocation rehab program typically includes:
- Phase 1 (0–3 weeks): Protection and pain control
- Sling use as recommended
- Gentle pendulum exercises
- Ice and manual therapy for pain and swelling
- Phase 2 (3–6 weeks): Restoring range of motion
- Guided mobility exercises
- Soft tissue work and joint mobilisation
- Postural correction
- Phase 3 (6–12 weeks): Strengthening
- Rotator cuff strengthening
- Scapular stabilisation exercises
- Progressive resistance training
- Phase 4 (3–6 months): Sport or activity-specific return
- Functional training
- Proprioception and neuromuscular control
- Sport-specific drills for athletes
Whether you visit our Pune clinic or prefer the convenience of our at-home physiotherapy service, our team designs a personalised programme based on which type of dislocation you had, your activity level, and your recovery goals.
Key Takeaways
- Anterior shoulder dislocation is far more common (~95%) and occurs when the arm is forced into abduction and external rotation. The shoulder takes on a squared-off appearance.
- Posterior shoulder dislocation is rare (~2–5%) but frequently missed. It often results from seizures or electric shock, and the arm is held in internal rotation.
- The most reliable clinical sign of a posterior dislocation is the inability to externally rotate the arm — not always an obvious deformity.
- On X-ray, anterior dislocations are usually obvious on an AP view. Posterior dislocations can appear nearly normal and require a lateral or axillary view to confirm. Look for the lightbulb sign and trough line.
- Both types require prompt reduction followed by a structured physiotherapy rehabilitation programme to restore strength, stability, and function.
- At Healyos Physiotherapy in Pune, we provide expert post-dislocation rehabilitation at our clinic and in the comfort of your home.
Frequently Asked Questions (FAQs)
1. Can a shoulder dislocate again after it’s been treated?
Yes, and recurrence is actually quite common — especially after an anterior dislocation in younger, active individuals. Studies show that recurrence rates can be as high as 50–90% in people under 25 who return to sport without proper rehabilitation. This is why structured physiotherapy, aimed at strengthening the rotator cuff and restoring joint stability, is so important. If recurrence is frequent, surgical options like a Bankart repair may be recommended.
2. How long does it take to fully recover from a shoulder dislocation?
Recovery time varies depending on the type of dislocation, how severe the soft tissue damage is, and whether there are associated fractures. In general, most people can return to light daily activities within 2–4 weeks. A return to sports or heavy lifting typically takes 3–6 months. Posterior dislocations, especially if missed early, may take longer to recover due to the complexity of the injury.
3. Is surgery always needed for shoulder dislocations?
Not necessarily. Most first-time dislocations are managed conservatively — reduction followed by physiotherapy. However, surgery may be recommended in cases of recurrent dislocation, significant bone loss (like a large Hill-Sachs or Bankart lesion), associated fractures, or when conservative treatment fails over multiple attempts. A specialist assessment is always recommended.
4. Can a posterior shoulder dislocation be missed for weeks or months?
Unfortunately, yes. This is a well-documented clinical problem. Because a posterior dislocation may not show clearly on a standard front-view X-ray, and because the shoulder deformity can be subtle, it is frequently misdiagnosed as a frozen shoulder, shoulder strain, or another condition. If you had a seizure or electric shock and your shoulder hasn’t been right since, ask your doctor specifically about the possibility of a posterior dislocation.
5. Should I use heat or ice after a shoulder dislocation?
In the first 48–72 hours after a dislocation or reduction, ice is generally recommended. It helps manage pain and reduce swelling. Apply for 15–20 minutes at a time with a cloth barrier to protect the skin. Heat may be introduced later in the rehabilitation phase (after acute swelling has settled) to help with muscle relaxation before exercises. Your physiotherapist will guide you on when to make the switch.

Leave a Reply